Light therapy is not the same as heat therapy; many people get this wrong from the very start.
Is light therapy the same as heat therapy? Many people misunderstand this from the very beginning; when first introduced to light therapy, they instinctively perceive it as a form of “heat-based treatment.”
They feel that it is only effective if they sense heat, and if they feel nothing, they doubt whether it is working at all.
However, an examination of the underlying mechanisms and clinical research reveals that this perception is fundamentally off-base.
Although light therapy and heat therapy often go hand in hand, they are essentially not the same thing.
To put it more accurately: light serves as a trigger, whereas heat is merely a potential byproduct.
Ⅰ Phototherapy and thermotherapy are essentially doing two different things.
Phototherapy essentially involves using light as an external stimulus to trigger a series of reactions within the cell.
These reactions can occur via entirely different pathways—such as chemical reactions, thermal effects, or the modulation of cellular signaling.
In contrast, thermotherapy is much simpler; its core mechanism is the elevation of temperature.
When tissue temperature rises to a certain range (typically above 40–45°C), it causes protein denaturation and cell membrane damage, thereby producing a therapeutic effect.
In other words, phototherapy focuses on “how to initiate a response,” whereas thermotherapy focuses on “producing results through temperature.”
Conceptually, the two operate at different levels.
Ⅱ The three types of phototherapy actually represent three completely different mechanisms.
In clinical practice, common forms of phototherapy can be broadly categorized into three types.
Photodynamic therapy (PDT) involves the photoactivation of a photosensitizer to generate reactive oxygen species (ROS), thereby causing oxidative damage to cells. Fundamentally a light-driven chemical reaction, this process relies heavily on the presence of oxygen (Cai et al., 2025; Li et al., 2020).
Photothermal therapy (PTT) directly converts light energy into thermal energy, killing cells through localized heating. Mechanistically, this process mirrors traditional hyperthermia, with the key difference being that light serves as the heat source (Kong & Chen, 2022; Han & Choi, 2021).
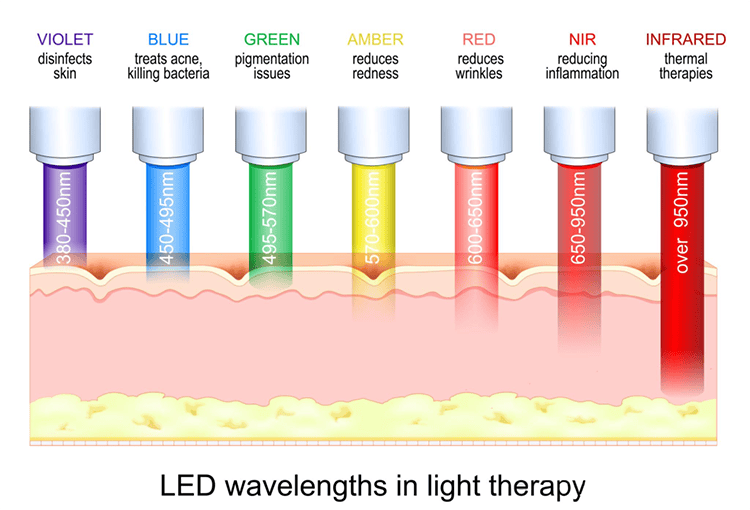
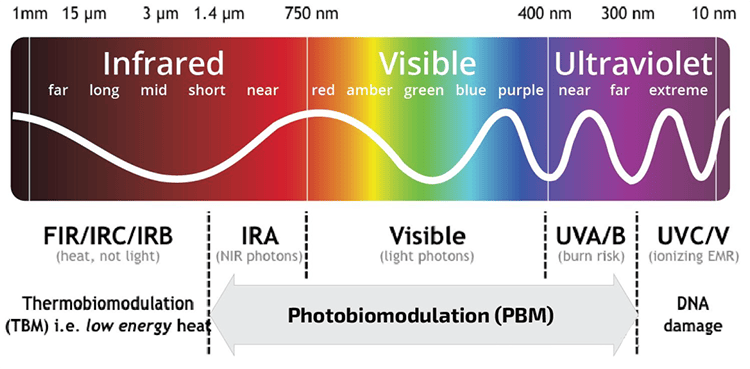
Meanwhile, the red-light masks or LED/low-level laser devices commonly encountered in daily life fall under the category of photobiomodulation (PBM). Rather than causing significant temperature increases, these therapies act on cellular structures—such as mitochondria—to modulate ATP production, Ca²⁺ signaling, and inflammatory states, thereby promoting repair and regulation (De Freitas & Hamblin, 2016).
Although all three methods utilize light, their mechanisms of action differ fundamentally.
III. Why do so many people conflate them?
A common misconception is to view all forms of light therapy simply as a type of “gentle heating.”
This misunderstanding is understandable, as everyday experience often equates “feeling something” with “being effective.”
However, this logic does not apply to light therapy.
For instance, photobiomodulation (such as red light masks, LEDs, or low-level lasers) generates almost no perceptible heat during normal use, yet it still triggers reactions at the cellular level; conversely, in photothermal therapy for tumors, a rise in temperature is a necessary condition.
In other words, while both involve light, some therapies rely on heat as a core mechanism, whereas others operate entirely independently of temperature.
Ⅳ Why this distinction is important in practice
First, it directly influences how we assess “effectiveness.”
Many people dismiss the efficacy of light therapy simply because they “don’t feel anything,” yet a lack of heat sensation is actually a characteristic feature of PBM.
In other words, the absence of sensation does not imply an absence of biological change.
Second, it relates to the understanding of safety parameters.
The risks associated with thermal therapy primarily stem from tissue damage caused by excessive heat, whereas photobiomodulation relies more heavily on a specific dosage window; exceeding this range can lead to inhibitory effects rather than the intended enhancement.
Finally, it determines the appropriate application scenarios for different technologies.
PDT or PTT is typically preferred when direct cell destruction is required, whereas PBM is more suitable for applications such as inflammation modulation and tissue repair.
Ⅴ In a clinical setting, they often exist in a “combinatorial relationship.”
In the field of cancer therapy, phototherapy and photothermal therapy are not mutually exclusive; rather, they are frequently used in combination.
For instance, combining photodynamic therapy and photothermal therapy with immunotherapy can enhance therapeutic efficacy at multiple levels while mitigating the emergence of drug resistance (Overchuk et al., 2023; Yi et al., 2024).
This further illustrates that they are fundamentally distinct mechanisms, rather than merely different manifestations of the same approach.
Phototherapy is not synonymous with thermotherapy.
Photothermal therapy is merely a subset of phototherapy and falls within the scope of thermotherapy;
In contrast, photodynamic therapy and photobiomodulation rely primarily on chemical reactions or the modulation of cellular signaling, rather than on raising temperature as the core mechanism.
The key concept to grasp is this:
Light serves as a triggering mechanism, whereas heat is simply one possible pathway of action.
Once this distinction is clarified, many questions regarding phototherapy—such as “Why do I feel nothing?” or “Why do results vary so much?”—become much easier to understand.


Leave a comment